DR. ALEJANDRO NOGUEIRA'S CLASSIFICATION OF THE TUBEROUS OR TUBULAR BREAST DEFORMITY | Given the polymorphism of the tuberous or tubular breasts and their different clinical aspects, based on his own personal experience Dr. Alejandro Nogueira proposes a new classification of tuberous or tubular breast he has designed, developed and applied, taking into account the different signs in a more detailed and organized manner, providing a therapeutic-clinical-prognostic approach with medico-legal perspectives.
CLINICAL PARAMETERS | In Dr. Alejandro Nogueira's classification the following parameters are taken into account with their corresponding gradation according to the anatomical and clinical features of the tuberous or tubular breast deformity.
Conicity (C) | The greater or lesser constriction of the breast cone | C0: none, no constriction, can have tuberous or tubular texture | C1: mild, one constrained quadrant | C2: moderate, two quadrants constrained | C3: severe, three quadrants constrained | C4: extreme, four quadrants constrained.
Areola (A) | Hypertrophy suffered by the areolar skin of the largest areola according to the anatomical proportions of the patient, measured as the radius gap between the outer areolar perimeter and the optimal one planned | A0: none, normal or hypoplastic areola | A1: mild, areola hypertrophied 1 cm | A2: moderate, areola hypertrophied 2 cm | A3: severe, areola hypertrophied 3 cm | A4: extreme, areola hypertrophied 4 cm.
Hernia (H) | The reducibility and shape memory of the areolar hernia | H0: none, no hernia or only manually provoked | H1: mild, reducible hernia with areolar contraction | H2: moderate, reducible hernia with underwear | H3: severe, manually reducible hernia | H4: extreme, irreducible hernia.
Submammary fold (F) | Downwards displacement from the original one the patient was born with necessary to achieve lower pole reconstruction and breast implant centricity | F0: in situ, without displacement, may require descent if there is an implant | F1: mild, displacement lesser than 2 cm | F2: moderate, displacement from 2 to 4 cm | F3: severe, displacement from 4 to 6 cm | F4: extreme, displacement larger than 6 cm.
Skin (S) | Neo lower pole, previously upper abdominal terrain, skin firmness | S0: none, flaccid | S1: mild, normal | S2: moderate, hard | S3: severe, very hard | S4: extreme, cuirass.
Associated problems (As) | Breast abnormalities, problems or issues, other than lack of development or breast hypoplasia, which require surgical correction at the same time than the tuberous or tubular breast deformity like pathological breast asymmetry, breast droopiness or mammary ptosis, breast hypertrophy or gigantomastia, previous breast surgeries, failed attempts of tuberous correction, presence of failed or ruptured breast implants and others | As0: none, no increase of complexity | As1: 1, mild increase of complexity | AS2: 2, moderate increase of complexity | As3: 3, severe increase of complexity | AS4: 4 or more, extreme increase of complexity.
GRADATION OF TUBEROSITY | Based on the previously classified clinical parameters the prognostic gradation and severity of the tuberous or tubular breast deformity is defined, combining them in different degrees of tuberous or tubular breast.
Tuberous or tubular breast grade 0 (trait): C0 + A0/1 + H0/1 + F0 + S0/1 | Tuberous or tubular breast grade I (mild): any combination with C1 or A2 or H2 or F1 | Tuberous or tubular breast grade II (moderate): any combination with C2 or A3 or H3 or F2 or S2 | Tuberous or tubular breast grade III (severe): any combination with C3 or A4 or H4 or F3 or S3 | Tuberous or tubular breast grade IV (extreme): any combination C4 or F4 or S4 | Complicated tuberous or tubular breast (X): any grade with As1/2/3/4.
SURGICAL RISK OF TUBEROSITY | A generic treatment prognosis criterion is concluded from this classification in terms of rates of complications and likelihood of a reoperation. These are overall percentages in an ideal scenario safe from the typical surgical complications, involving highly adherent implants, enjoying a well trained surgeon and done on strictly collaborative patients.
Very low risk (5%): grade 0 | Low risk (10%): grades I and II | Medium risk (15%): grade III or grades 0/I/II-X | High risk (20%): grade IV or grade III-X | Very high risk (25%): grade IV-X.
To these percentages has to be added another 25% probability of poor result and reintervention when poorly adherent implants are used and an additional 25% in case the surgeon is not experienced in tuberous or tubular breast treatment techniques. An extra 10% risk would source from any usual postoperative complication, including non compliant patient of postoperative immobility.
This series of tuberous or tubular breast patients depicts different configurations of the deformity so that the polymorphism of this congenital abnormality is shown; each case has been tagged following Dr. Alejandro Nogueira's classification for a better understanding how it works and aiming to provide the surgical prognosis of each case.
READ LESS









































































































































































 Sending vote...
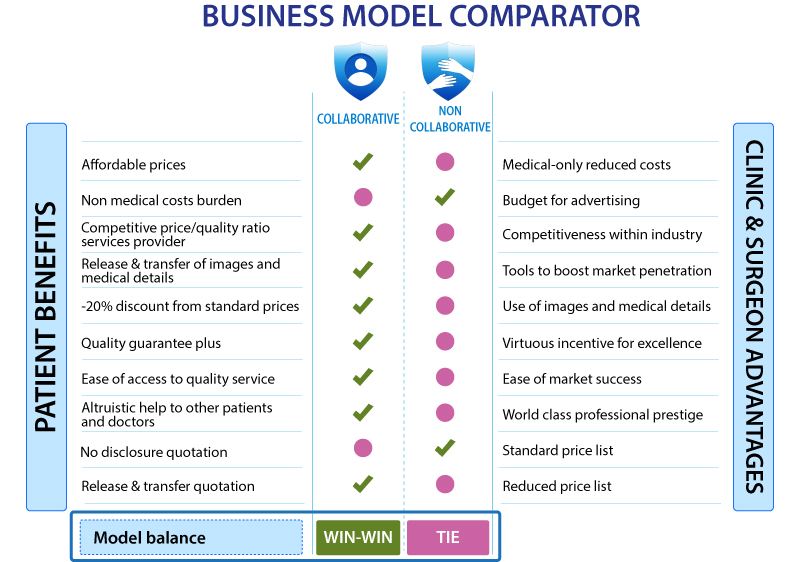
Sending vote... READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL

 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840







































































































































































































































































































































































































































































































